
A new research study done by a group of researchers in Japan was published in The Orthopaedic Journal of Sports Medicine examining the effects of bracing on the ulnar collateral ligament (the tommy john ligament)( Hattori, Akasaka, Otsudo, Takei, & Yamamoto, 2017).
Background: It’s fair to assume at this point pretty much everyone knows pitching is stressful on the elbow. The elbow contains a ligament on the medial (inside) side called the ulnar collateral ligament. The ulnar collateral ligament is responsible for maintaining the stability of the elbow during throwing. The ligament is composed of two bundles: an anterior (frontwards) and posterior (towards the back). Of these two bundles, the anterior portion has been found to be the more important of the two when it comes to throwing a baseball. In a cadaver study using ultrasound to determine how much instability occurs when releasing these structures, the anterior band of the anterior bundle proved to be the most important structure: “Release of the anterior band of the anterior bundle resulted in a mean Δ of 2.0 mm (95% CI, 1.1-2.8 mm). Release of the posterior band of the anterior bundle resulted in a mean Δ of 1.4 mm (95% CI, 0.6-2.2 mm). Release of the entire anterior bundle caused a mean increase in ulnohumeral valgus joint gapping of 3.4 mm (95% CI, 2.4-4.3 mm). Release of the remaining individual structures each resulted in a mean increase in valgus joint gapping of ≤0.8 mm” (Ciccotti, Hammoud, Dodson, Cohen, Nazarian, & Ciccotti, 2014). If the wording confused you, the anterior bundle is combined two parts called the anterior and posterior bands. As you can see from the results, releasing the anterior band of the anterior bundle resulted in the largest increase in elbow gapping. Elbow gapping increases overtime with pitching. In a study on 40 professional baseball pitchers without a history of elbow injury, Ellenbecker, Mattalino, Elam,& Caplinger, (1998) found, “The dominant extremity, on average, had 0.32 +/- 0.42 mm greater medial joint width increases with application of the valgus stress”. With applied stress the throwing arm opened to 4.72 +/- 1.23 mm and the non-throwing arm opened to 4.46 +/- 0.8 mm. In a very similar study, Ciccotti, Atanda, Nazarian, Dodson, Holmes, & Cohen (2014) used ultrasound to look at changes in the ulnar collateral ligament associated with pitching in 368 asymptomatic pitchers. Elbow gapping was significantly greater in the throwing arm with stress applied: “The mean joint space width at rest was 3.32 mm in the dominant elbow and 2.94 mm in the nondominant elbow. The difference was not statistically significant. When stress was applied, however, the mean joint space width of the dominant elbow was significantly greater (P < .003) than that of the nondominant elbow, with values of 4.56 mm and 3.72 mm, respectively”(Ciccotti, Atanda, Nazarian, Dodson, Holmes, & Cohen, 2014). Overall, the difference from rest was, “1.24 mm in the dominant elbow and 0.78 mm in the nondominant elbow (P ≤ .004)”(Ciccotti, Atanda, Nazarian, Dodson, Holmes, & Cohen, 2014). This difference between rest and stress conditions was very similar to the Ellenbecker study whom found differences of 1.20 mm in the throwing arm and 0.88 mm in the nonthrowing arm (Ellenbecker, Mattalino, Elam,& Caplinger, 1998). There are some small differences in the numbers which are most likely due to the rather large sample size in the Ciccotti study and a small difference in the placement of the elbow while measuring (25 v 30 degrees of flexion) and body positioning.
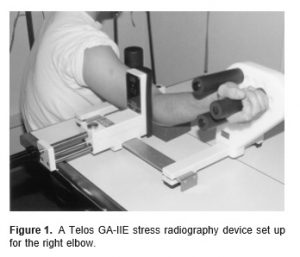
Stress ultrasound setup of the Ellenbecker study, 25 degrees of elbow flexion and the arm abducted to ~90 degrees (Ellenbecker, Mattalino, Elam,& Caplinger, 1998)
Stress ultrasound set up in the Ciccotti study, with the elbow flexed to 30 and arm in ~ 90 degrees of flexion (Ciccotti, Atanda, Nazarian, Dodson, Holmes, & Cohen, 2014)
As you probably noticed, all these numbers have been found in professional pitchers. What kind of results can be expected in younger populations? (To note both groups in the two above studies were pretty young, with both average ages being around 22 years old). SASAKI, TAKAHARA, OGINO, KASHIWA, ISHIGAKI, & KANAUCHI (2002), examined thirty college level baseball players. The mean age of the players was 21.7 years old with an average playing experience of 10.5 years. Twelve of the subjects were pitches and eighteen were fielders. Thirteen of the subjects had complained of medial elbow soreness at some point in their playing career. Unlike, the prior two studies mentioned, this study used a gravity dependent position of the arm at 90 degrees abduction and 90 degrees of elbow flexion and the degrees of external rotation unknown (important for later on) (pictured).
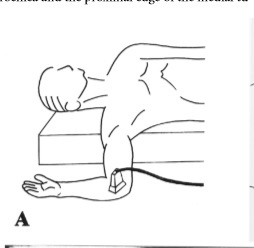
Stress ultrasound in the 90/90 gravity dependent position (SASAKI, TAKAHARA, OGINO, KASHIWA, ISHIGAKI, & KANAUCHI, 2002)
This position is believed to be advantageous for evaluating the ulnar collateral ligament’s contribution to elbow stability because it minimizes the contribution from bone, “In contrast, we placed the elbow in 90° of flexion during the gravity stress test. When the elbow is flexed 90°, the contribution of the ulnar collateral ligament with regard to constraining the elbow against valgus stress becomes large and the contribution of the osseous articulation becomes small” (SASAKI, TAKAHARA, OGINO, KASHIWA, ISHIGAKI, & KANAUCHI, 2002). The average joint gapping reported in this study was 2.7 mm on the throwing arm versus 1.6 mm on the non-throwing arm which was statistically significant, with a mean difference of 1.1 mm (p<0.01) (SASAKI, TAKAHARA, OGINO, KASHIWA, ISHIGAKI, & KANAUCHI, 2002). This leaves us with elbow gapping of:
Ellenbecker, Mattalino, Elam,& Caplinger, (1998): 4.72mm / average difference: 0.32 mm
Ciccotti, Atanda, Nazarian, Dodson, Holmes, & Cohen (2014): 4.56 mm / average difference: 0.84 mm
SASAKI, TAKAHARA, OGINO, KASHIWA, ISHIGAKI, & KANAUCHI (2002): 2.7 mm / average difference: 1.1 mm
Looking at the results from these 3 studies you can see quite a bit of variation, with the Ellenbecker and Ciccotti studies being pretty close in joint gapping, but with their mean differences being pretty far apart. The Sasaki study had much less overall gapping, but had the largest difference, and was closer to the Ciccotti average difference.
Now that we have our relative baselines, let’s get into the effects of elbow bracing on joint space.
Study: Hattori, Akasaka, Otsudo, Takei, & Yamamoto (2017), examined the effects of an elbow brace on medial elbow joint space.
Subjects: Twenty-five high school pitchers were selected for the study. The study design was a within participant cross-over, meaning each subject pitched in a randomized order once with the brace and once without the brace. The subjects averaged 16.6 years old and have been playing baseball for an average of 8.8 years. Participants were healthy without a history of elbow/shoulder pain.
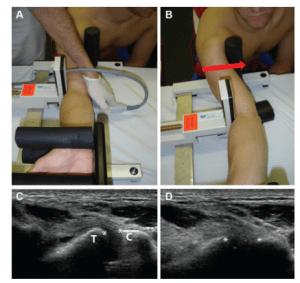
Materials and Methods: The subjects threw 100 pitches (all fastballs) in sets of 20 pitches (5 sets) with 15 seconds of rest between pitches. There was a 1 week rest period between the 2 sessions. The elbow brace consists of 3 valgus suppression straps and was fitted to each individual (JAPAN, Sigmax). The ultrasound evaluation was done in a gravity dependent position, similar to the Sasaki study, with the difference being the subject was placed in maximal external rotation: “Participants were placed supine on the bed with the shoulder in 90 of abduction, 0 of horizontal abduction, and maximum external rotation; the elbow in 90 of flexion; and the forearm in neutral position. The elbow joint lay off the side of the bed” (Hattori, Akasaka, Otsudo, Takei, & Yamamoto, 2017). The elbow joint space was measured pre-throwing, and then in between each set of pitches. 
(Hattori, Akasaka, Otsudo, Takei, & Yamamoto, 2017)
Stress ultrasound in the 90/90 position at max external rotation. Does forcing the subject into max external rotation significantly increase elbow gapping? My thoughts are yes!
Results: Elbow joint gapping significantly increased in the control group after 60 pitches (p<0.01). The elbow brace did not experience an increase in joint gapping. Comparing the two groups, the elbow brace significantly reduced joint gapping after 60 pitches (p<0.01). There was a small dip in velocity (nonsignificant) when wearing the brace. Accuracy of pitching was unaffected (number of strikers per 20 pitches).
Here are the joint gapping numbers per set (mm):
Brace: 5.02 ± 0.74, 5.09 ± 0.73, 5.12 ± 0.75, 5.14 ± 0.77, 5.16 ± 0.77, 5.17 ± 0.83
Control: 4.97 ± 0.90, 5.23 ± 0.90, 5.52 ± 0.84, 5.83 ± 0.91, 6.01 ± 1.08, 6.22 ± 1.06
The control group increased from 4.97 mm to 6.22 mm (1.25 mm) and the brace increased 0.15 mm.
Discussion: This study certainly presents some interesting findings. At first glance, the amount of gapping found seems quite large. Here are the numbers:
Ellenbecker, Mattalino, Elam,& Caplinger, (1998): 4.72mm average difference: 0.32 mm
Ciccotti, Atanda, Nazarian, Dodson, Holmes, & Cohen (2014): 4.56 mm average difference: 0.84 mm
SASAKI, TAKAHARA, OGINO, KASHIWA, ISHIGAKI, & KANAUCHI (2002): 2.7 mm average difference: 1.1 mm
Hattori, Akasaka, Otsudo, Takei, & Yamamoto (2017): 4.97 mm (pre-pitching), 6.22mm post-pitching
As you can see, this study found the largest amount gapping. This could mean a few things. First, the positioning of the subject was in the 90/90 position with maximal external rotation. It is conceivable this position results in the most joint play. The Sasaki study also used a 90/90 position, but the amount of external rotation was not mentioned. There is a large discrepancy between these two studies (2.7 mm v 4.97 mm). Are the samples that much different (collegiate v high school) or does the potential (remember we don’t know) increase in external rotation make that large of a difference? Second, it appears pitching causes a temporary increase in elbow joint laxity to go with the long term changes found in the 3 previously mentioned studies. It would be interesting to see a follow-up ultrasound to determine when the joint gapping returns to normal. This could have serious implications for pitching back to back days and for throwing in general. This assumes that throwing with more laxity would increase the chance for injury. The significant increase resulted after 60 pitches were thrown, keep that in mind as well. Third, and lastly, does preventing this increase in laxity actually reduce stress on the elbow? We don’t know as force was not directly measured. And does it reduce force enough to significantly reduce injury rates? Driveline (an awesome baseball reference) did an in-house study and actually found an increase amount of elbow stress using a different brace, which I won’t get into, simply go read the awesome article. The brace appears from the outside to be different than the brace presented above. The EpiTrain brace is intended to limit hyperextension, while the Sigmax intends to limit the amount of valgus stress. Both braces seem a bit clunky and bulky, I’d like the braces to be made slimmer. The Sigmax brace did slightly reduce velocity.

The Sigmax brace (Hattori, Akasaka, Otsudo, Takei, & Yamamoto, 2017)

Epitrain brace taken from DrivelineBaseball
Ciccotti, M. C., Hammoud, S., Dodson, C. C., Cohen, S. B., Nazarian, L. N., & Ciccotti, M. G. (2014). Stress Ultrasound Evaluation of Medial Elbow Instability in a Cadaveric Model. The American Journal of Sports Medicine, 42(10), 2463-2469. doi:10.1177/0363546514542805
Ciccotti, M. G., Atanda, A., Nazarian, L. N., Dodson, C. C., Holmes, L., & Cohen, S. B. (2014). Stress Sonography of the Ulnar Collateral Ligament of the Elbow in Professional Baseball Pitchers. The American Journal of Sports Medicine, 42(3), 544-551. doi:10.1177/0363546513516592
Ellenbecker, T., Mattalino, A., Elam, E., & Caplinger, R. (1998). Medial Elbow Joint Laxity in Professional Baseball Pitchers. The American Journal of Sports Medicine, 26(3).
Harada, M., Takahara, M., Maruyama, M., Nemoto, T., Koseki, K., & Kato, Y. (2014). Assessment of medial elbow laxity by gravity stress radiography: comparison of valgus stress radiography with gravity and a Telos stress device. Journal of Shoulder and Elbow Surgery, 23(4), 561-566. doi:10.1016/j.jse.2014.01.002
Hattori, H., Akasaka, K., Otsudo, T., Takei, K., & Yamamoto, M. (2017). The Effects of Elbow Bracing on Medial Elbow Joint Space Gapping Associated With Repetitive Throwing in High School Baseball Players. Orthopaedic Journal of Sports Medicine, 5(4), 232596711770236. doi:10.1177/2325967117702361
SASAKI, J., TAKAHARA, M., OGINO, T., KASHIWA, H., ISHIGAKI, D., & KANAUCHI, Y. (2002). ULTRASONOGRAPHIC ASSESSMENT OF THE ULNAR COLLATERAL LIGAMENT AND MEDIAL ELBOW LAXITY IN COLLEGE BASEBALL PLAYERS. The Journal of Bone and Joint Surgery-American Volume, 84(4), 525-531. doi:10.2106/00004623-200204000-00003